When Daniel Carlat, a psychiatrist in Massachusetts, was flown to New York with his wife by Wyeth, the “training” weekend he attended in a luxury hotel was topped off with a Broadway show. It was early 2001 and he had just agreed to the US pharmaceuticals company’s proposal that he give talks to doctors about its antidepressant Effexor.
During the following year, he was regularly paid fees of $750 a time to drive to “lunch and learn” sessions where he would speak for 10 minutes to emphasise the drug’s advantages to fellow doctors, using slides prepared by the company. “It seemed like a win-win,” he recalls. “I was prescribing it, educating doctors and making some money.”
But within a few months, he became disillusioned with his co-option as a marketing representative. He was selectively presenting clinical data that put the drug in a positive light to physicians who had been targeted by the company through “data mining” techniques that identified their individual prescription patterns.
Category: Health/Fitness
Teddy, J.P. and Henry
The last seven years have had much in common with the period of 1893 to 1900. But the turmoil this country experienced during the first few years of the 20th century also seems to be mirrored in the events of today.
Certainly the nation once witnessed the rise of the more radical elements, whether they were far-left anarchist movements or center-left progressives. Those movements attested to a very real battle being waged for the heart and soul of what the American Century would become. Its apex was marked by one president’s assassination and by the dreams of an inventor who wanted to revolutionize our mobility.
Given what has transpired over the last two years, it is haunting to read Teddy Roosevelt’s letter to Congress and his personal thoughts on companies whose sole reason for existence is to make their owners wealthy without regard to the damage they were doing to society. One wonders what would have happened if today’s Wall Street Masters of the Universe had been confronted in a White House with the same resolve that Roosevelt showed to J.P. Morgan.
Community Yoga

What should medicine do when it can’t save your life?
Modern medicine is good at staving off death with aggressive interventions—and bad at knowing when to focus, instead, on improving the days that terminal patients have left.
Sara Thomas Monopoli was pregnant with her first child when her doctors learned that she was going to die. It started with a cough and a pain in her back. Then a chest X-ray showed that her left lung had collapsed, and her chest was filled with fluid. A sample of the fluid was drawn off with a long needle and sent for testing. Instead of an infection, as everyone had expected, it was lung cancer, and it had already spread to the lining of her chest. Her pregnancy was thirty-nine weeks along, and the obstetrician who had ordered the test broke the news to her as she sat with her husband and her parents. The obstetrician didn’t get into the prognosis—she would bring in an oncologist for that—but Sara was stunned. Her mother, who had lost her best friend to lung cancer, began crying.
The doctors wanted to start treatment right away, and that meant inducing labor to get the baby out. For the moment, though, Sara and her husband, Rich, sat by themselves on a quiet terrace off the labor floor. It was a warm Monday in June, 2007. She took Rich’s hands, and they tried to absorb what they had heard. Monopoli was thirty-four. She had never smoked, or lived with anyone who had. She exercised. She ate well. The diagnosis was bewildering. “This is going to be O.K.,” Rich told her. “We’re going to work through this. It’s going to be hard, yes. But we’ll figure it out. We can find the right treatment.” For the moment, though, they had a baby to think about.
Fabulous: Health Care Video Stream with Campaign Contributions…
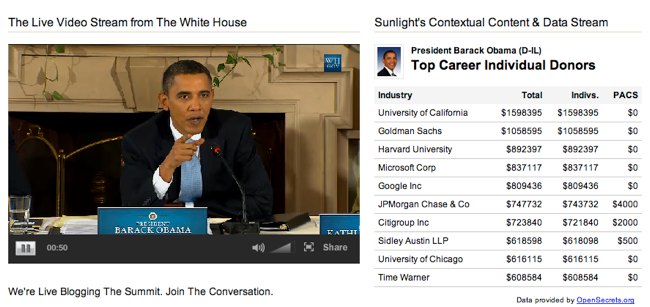
The Sunlight Foundation provides a great service here.
The Legacy of Billy Tauzin: The White House-PhRMA Deal
More than a million spectators gathered before the Capitol on a frosty January afternoon to witness the inauguration of Barack Obama, who promised in his campaign to change Washington’s mercenary culture of lobbyists, special interest influence and backroom deals. But within a few months of being sworn in, the President and his top aides were sitting down with leaders from the pharmaceutical industry to hash out a deal that they thought would make health care reform possible.
Over the following months, pharmaceutical industry lobbyists and executives met with top White House aides dozens of times to hammer out a deal that would secure industry support for the administration’s health care reform agenda in exchange for the White House abandoning key elements of the president’s promises to reform the pharmaceutical industry. They flooded Congress with campaign contributions, and hired dozens of former Capitol Hill insiders to push their case. How they did it—pieced together from news accounts, disclosure forms including lobbying reports and Federal Election Commission records, White House visitor logs and the schedule Sen. Max Baucus releases voluntarily—is a testament to how ingrained the grip of special interests remains in Washington.
Throwing Computers At Healthcare
Computerworld reports on an extensive new Harvard Medical School study, appearing in the American Journal of Medicine, that paints a stark and troubling picture of the essential worthlessness of many of the computer systems that hospitals have invested in over the last few years. The researchers, led by Harvard’s David Himmelstein, begin their report by sketching out the hype that now surrounds health care automation:
Enthusiasm for health information technology spans the political spectrum, from Barack Obama to Newt Gingrich. Congress is pouring $19 billion into it. Health reformers of many stripes see computerization as a painless solution to the most vexing health policy problems, allowing simultaneous quality improvement and cost reduction …
In 2005, one team of analysts projected annual savings of $77.8 billion, whereas another foresaw more than $81 billion in savings plus substantial health gains from the nationwide adoption of optimal computerization. Today, the federal government’s health information technology website states (without reference) that “Broad use of health IT will: improve health care quality; prevent medical errors; reduce health care costs; increase administrative efficiencies; decrease paperwork; and expand access to affordable care.
Medical Tourism Takes Flight
A growing number of U.S. insurers are paying for patients to have medical procedures performed more cheaply overseas. And that’s raising the profile of a few companies you’ve probably never heard of. Video: Bangkok Bypass Surgery
IN THE PAST THREE MONTHS, THE CREAKY Barron’s staff has replaced a hip, two knees and undergone various nips and tucks. Based on average prices, these cost a total of at least $100,000. But abroad, say in Singapore, the tab would have been about $50,000, including stays in a private room, airfare and a vacation for the patients and their companions. Elsewhere in Asia, medical care is even cheaper. That’s why more U.S. insurers are considering financing treatment for Americans willing to travel abroad. In fact, “medical tourism” could help rein in the health-care costs that devour 16% of America’s gross domestic product.
That possibility is raising the profile of a few publicly traded companies you’ve probably never heard of: Thailand’s Bumrungrad Hospital (ticker: BH.Thailand) and Bangkok Dusit Medical Services (BGH.Thailand), Singapore’s Parkway Holdings (PWAY.Singapore) and Raffles Medical (RFMD.Singapore), and India’s Apollo Hospitals (APHS.India). Says Prathap Reddy, the U.S.-trained cardiologist who founded Apollo in 1983 and is its chairman: “We bring excellent care at a cost benefit. If the U.S. were to cover all its people, there would be a demand/supply gap. India can step in with equivalent care at one-fifth the cost.”
Britain’s National Medical Records Project – “No money spent on training”…
“If you live in Birmingham,” declared Tony Blair when he was UK prime minister, “and you have an accident while you are, for example, in Bradford, it should be possible for your records to be instantly available to the doctors treating you.”
Not any more. Or not, at least, if the Conservatives win the next general election. For the Tories have pledged to scrap the country-wide version of the National Health Service’s electronic patient record.
Back in 2002, the idea of a full patient record, available anywhere in an emergency, was the principal political selling point for what was billed as “the biggest civilian computer project in the world”: the drive to give all 50m or so patients in England (the rest of the UK has its own arrangements) an all-singing, all-dancing electronic record. Roll-out was meant to start in 2005 and be completed by 2010.
Under a Conservative government, development of the local record – exchangeable between primary care physicians and their local hospitals – would continue. Nationally, clinicians would still be able to seek access to it when needed from the doctors who would hold it locally. But the idea of a national database of patients’ records, instantly available in an emergency from anywhere in the country, would disappear.
This may or may not matter, depending on your point of view. For many clinicians, the idea of an instantly available national record was always something of a diversion. It is access to a comprehensive record locally that is crucial for day-to-day care.
Nonetheless, the Conservatives’ decision to scrap the central database is a symbolic moment for a £12bn ($20bn, €14bn) programme that has struggled to deliver from day one. It is currently running at least four years late – and there looks to be no chance in the foreseeable future of its delivering quite what was promised.
…..On top of that, while there was a £6bn budget for the 10-year central contracts, no money was earmarked for training, in spite of the lesson, from the relatively few successful installations of electronic records in US hospitals, that at least as much has to be spent on changing the way staff work as is spent on the systems themselves.
The Machinery Behind Health-Care ReformHow an Industry Lobby Scored a Swift, Unexpected Victory by Channeling Billions to Electronic Records
When President Obama won approval for his $787 billion stimulus package in February, large sections of the 407-page bill focused on a push for new technology that would not stimulate the economy for years.
The inclusion of as much as $36.5 billion in spending to create a nationwide network of electronic health records fulfilled one of Obama’s key campaign promises — to launch the reform of America’s costly health-care system.
But it was more than a political victory for the new administration. It also represented a triumph for an influential trade group whose members now stand to gain billions in taxpayer dollars.
A Washington Post review found that the trade group, the Healthcare Information and Management Systems Society, had worked closely with technology vendors, researchers and other allies in a sophisticated, decade-long campaign to shape public opinion and win over Washington’s political machinery.
Automation certainly makes sense, but we taxpayers should not be subsidizing it….